|
Periodontal Reconstructive Bone Surgery for Bone Defect Therapy |

A bone defect is a "concavity of this tissue that surrounds one or more teeth, in the districts in which the most appropriate form should be the convex one".
Bone defects are classified according to the residual walls:
three, two, one wall, four walls, better circumferential and combined bone defects (when there are more combinations of walls).
In these cases the therapy can only be reconstructive with grafts.
The most commonly used grafting material is bone.
Autogenous bone taken from the same patient can be used (Petti 1985). In some cases the extent of the defects suggests the use of non-autologous material.
Over time, Kiel's bone (Petti 1986), a deproteinated bovine bone, has been used. Going forward in time, artificial materials were used, reabsorbed as sintered tricalcium tricalcium hexaphosphate, which transfers calcium and phosphates used by the new bone.
Non-resorbable artificial materials such as hydroxyapatite (Petti 1986). And again the calcium sulfate which is very current and is a synthesis of "functioning" of the first two.
A full-thickness flap is sculpted.
The bone defect is highlighted and it is cruelly to put in communication the underlying spongy with the graft.
It precedes the graft by condensing the bone into the defect.
Once the defect is filled, the graft is shaped
If desired, the PRP, PRF can be mixed into the graft to take advantage of its strong tissue stimulation action to promote osteogenesis. (See "Regeneration with Membranes")
Or with amelogenins, hyaluronic acid, calcium sulphate, calcium phosphates etc.
At the end of a bone grafting procedure, the flap with detached stitches is sutured as a rule. |
Regenerative Periodontal Bone Surgery with Membranes |
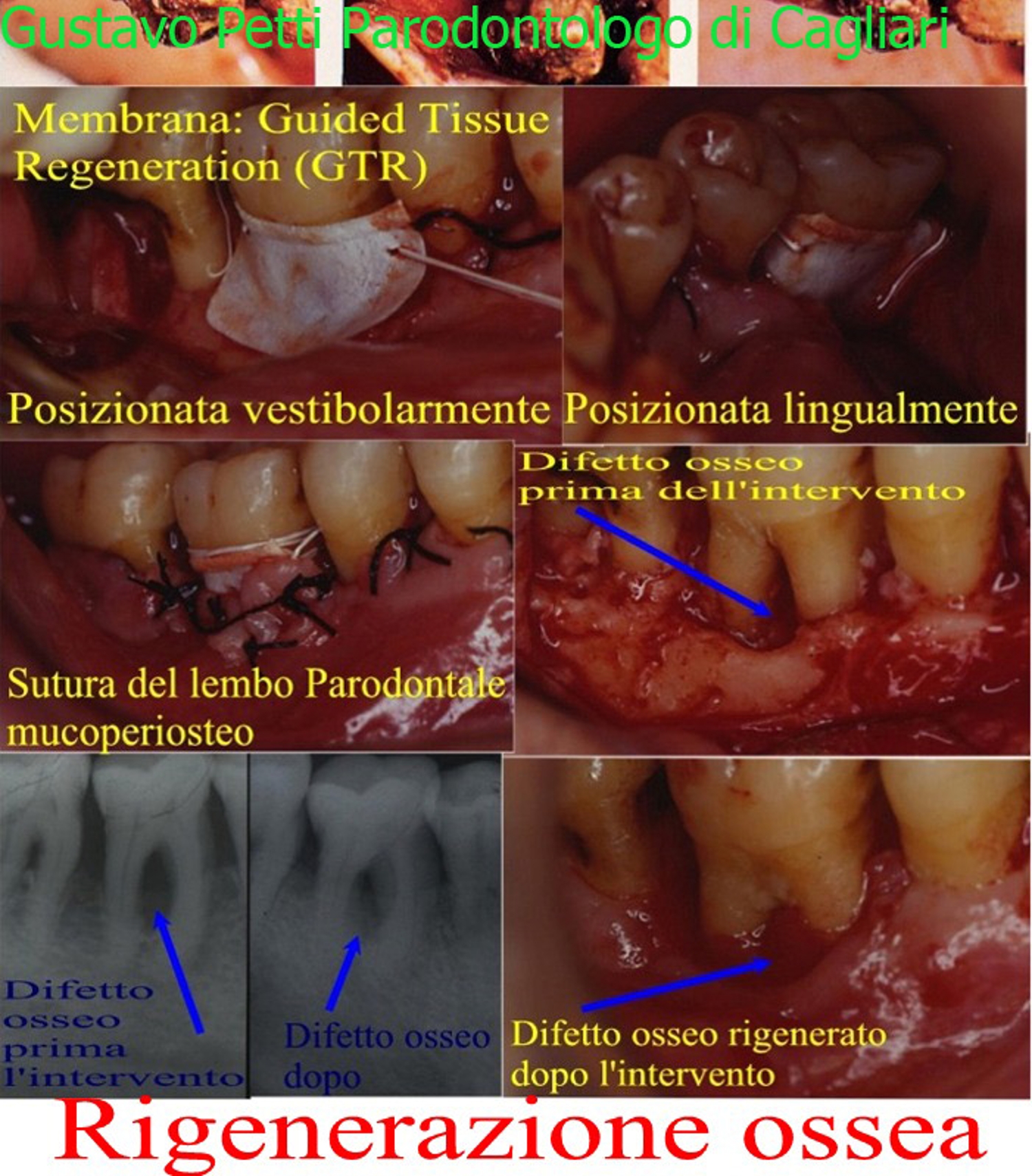
Deep Parodontal Regenerative Bone Surgery for the Therapy of a Third Passage Class Bone Defect of a Molar Inferior with the use of Membranes with GBR Methods (Guided Bone Regeneration) and GTR (Guided Tissue Regeneration = Tissue Regeneration) Guided) and PRP and PRF with Release of Grow Factors = Growth Factors. |
| Mucogingival surgery for the treatment of gingival recessions |
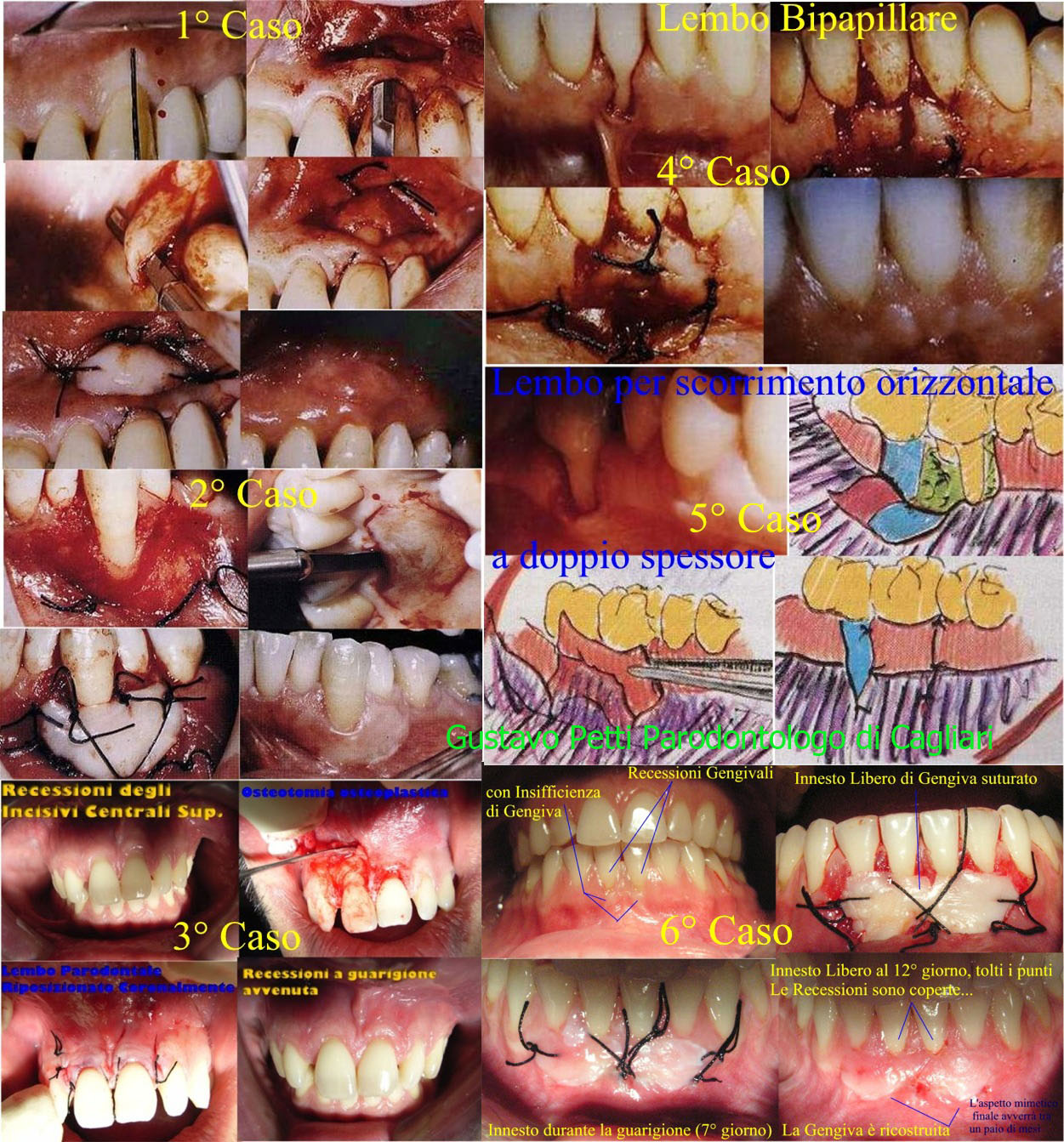
(Examples of the many interventions available)
Coronally Repositioning Flap with Free Gingiva Grafting (personal variant of the Tarnow Semilunar Flap). Then, Bipapillary Flap, Flap for Horizontal Scroll, Free Gingiva Graft with Blending of the Same Graft. Then flap for horizontal double-wide scrolling. Then Flap Repositioning Coronally in 11 and Tarnow's Fledgling Flap, Modified with Personal Technique in 21. Then, Increase in the Fornice with a Double Free Graft of Adherent Gingiva. |
| Gnathology |
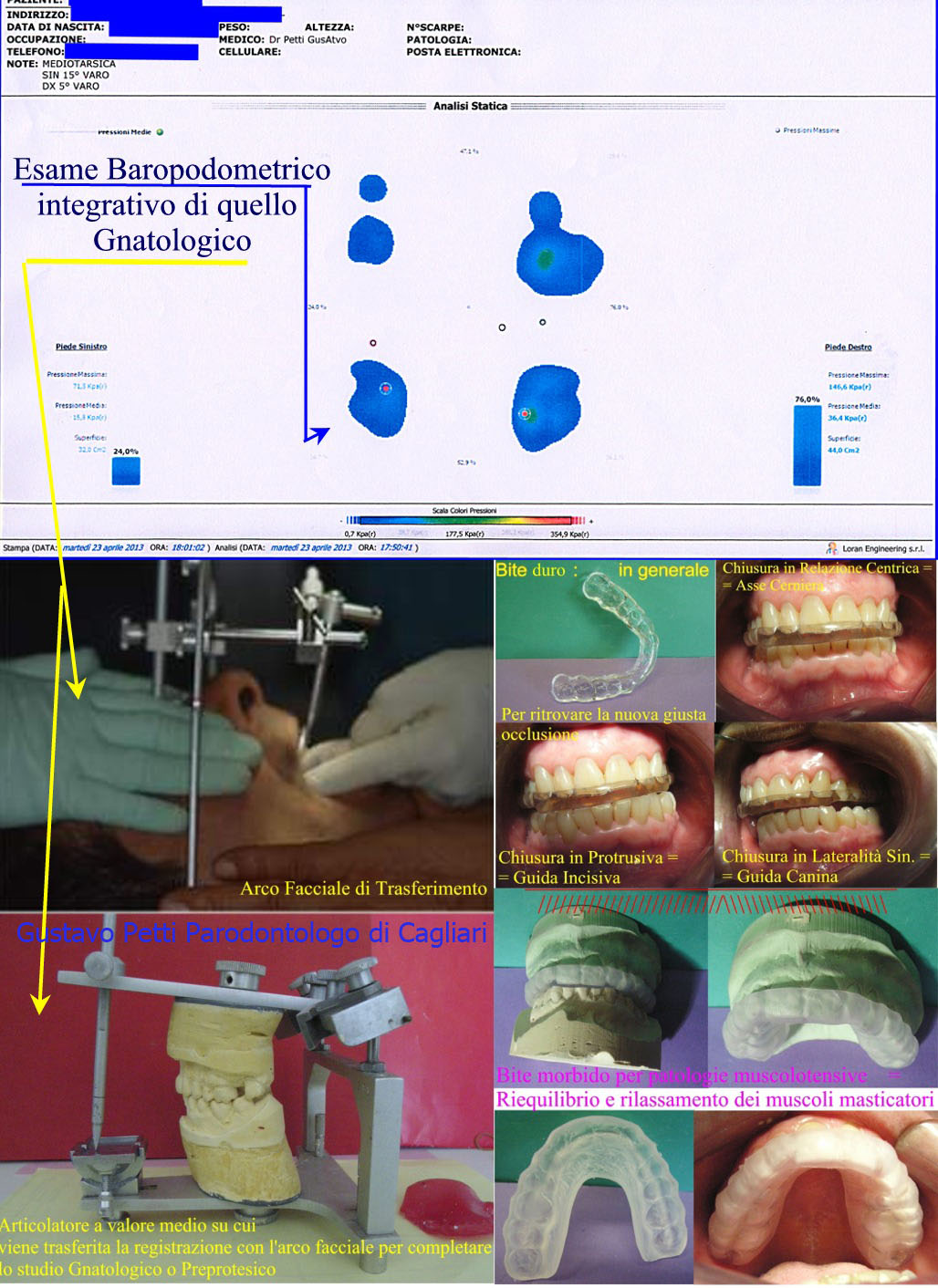
Computerized Stabilometric Examination
Facial Arch of Transfer to Detect the Spatial Relations of the Two Dental Arches with the Cranial Base and Assembly on Medium Value Articulator for the Study, among other Parameters, of the Angle and Movement the Bennets between the Sagittal Plane and the Condylar Movement of the Jaw in Laterality for the Evaluation of the Functions and Dysfunctions of the Working Side and of the Non Working Part of the Test of the Condiles.
Bite Plane (various ipi), Diagnostic, Symptom, Therapetico. The Teapeutico makes the Brain forget the current gnathological pathological position, making it a "Tabula Rasa" that allows to find the original Gnathological Position to Rehabilitate the Right Gnathology and Occlusion! |
| Retrograde |
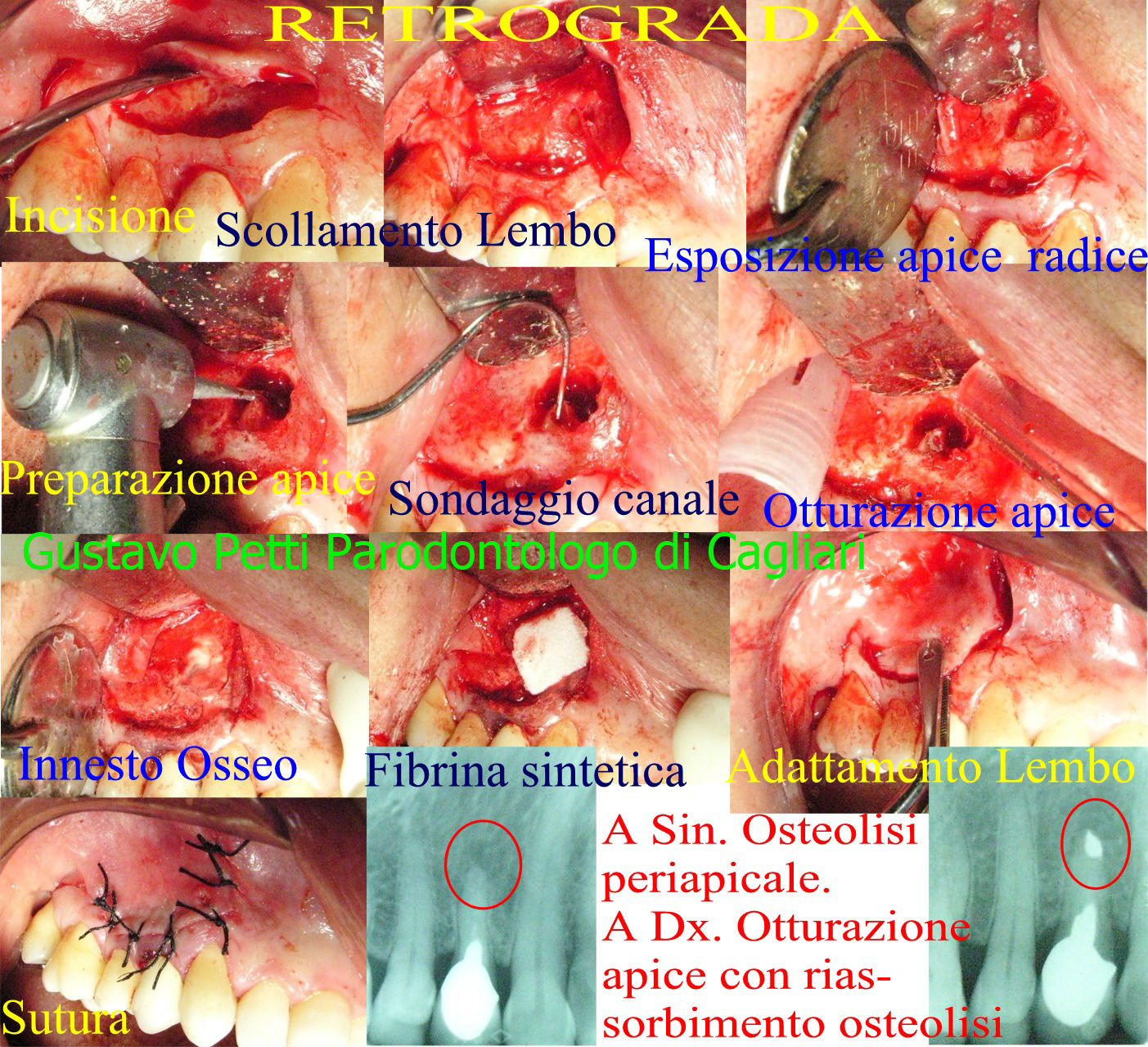
Conceptually, the Microbes inside the Root send their Toxins out to the bone, to which the organism responds with the formation of Periapical Osteolysis (Granuloma or Cysts), in order to contain the same infection and to defend itself. Removed the Microbes with the Endodontic Therapy, through "Normal" Orthograde or, if in presence of Obstacles (as in this case shown), through Retrograda Chirurgica, the Toxins are not more Emesse and the zone of Periapical Osteolysis, it Reassumes!
Retrograde is a surgical intervention very different from Apcectomia, which belongs to the Middle Ages of Dentistry because it does not seal the apex, shortens the root and weakens it and opens the way to recurrence. With Retrograde, instead, the Flute Beak Apex opens to enter and retrograde the apical canal itself, which is then sealed with MTA or Zinc-free Surgical Amalgama because it is not hygroscopic or with other materials! |
| Gingivectomy |
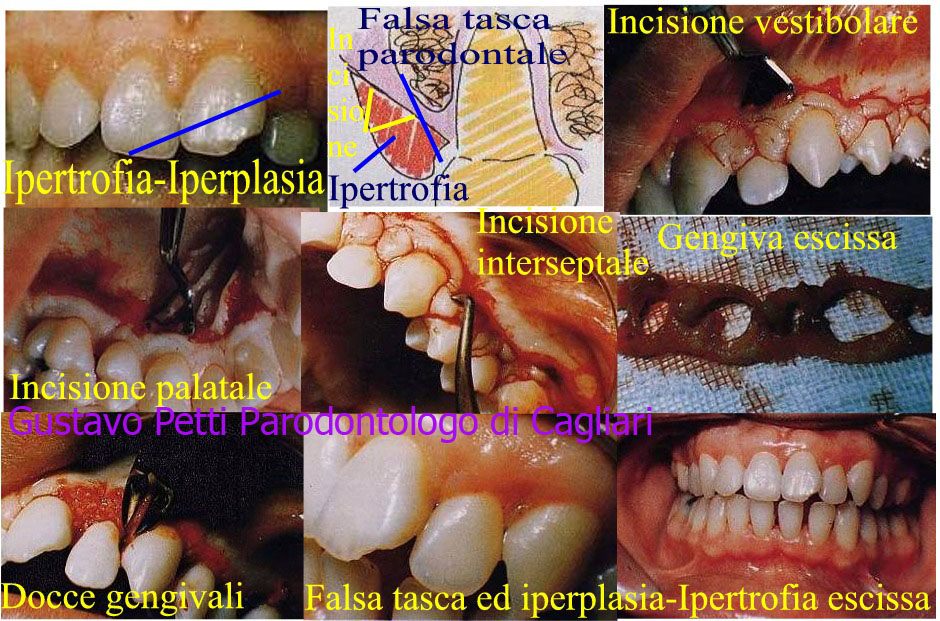
Gingivectomy in Bisello terno for the Treatment of a Hypertrophy-Gingival Hyperplasia by Difeilidantoina in Epileptic Paziene.
Gingial hypertrophy creates the formation of a False Pocket Pardontal, very different from the Periodontal pocket. In this Last, there is a Detachment of the Epithelial and Connective Attack of the Gingiva, from the Tooth, while in the first one, this detachment is not there and the Tasca seems Such only because there is more Gingiva, that is Hypertrophic, for this is called Falsa Tasca. The Periodontal pocket is the expression of a periodontitis (Piorea Volgarmente). The False Tasca, as in this case, is instead the manifestation of a hypertrophy-gingival hyperplasia! |
| Periodontal lesions or fractures of bifurcations |
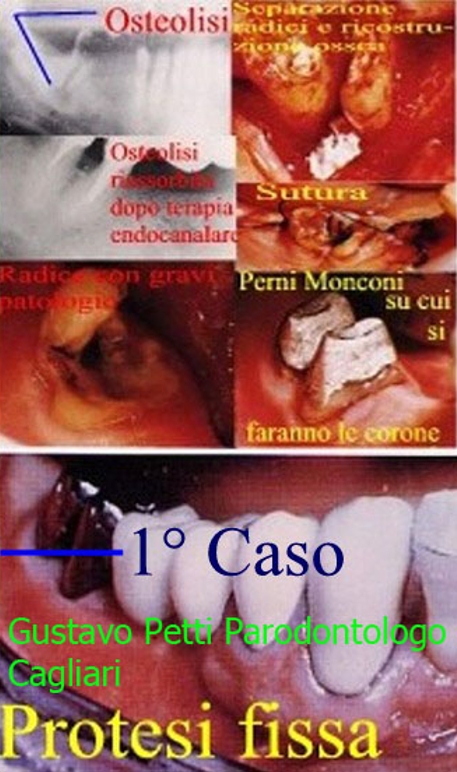
The Roots of a lower Molar are separated with a Parodtale Bone Defect of the Third Passing Class.
Rebuilds the Bone Diftto with Kiel Heterologous Bone Graft, deproteinate because it has no Antigen power.
It proceeds to Endodntica Therapy and rehabilitates each of the Two Radci with a Pin-Stump in Gold (as in this case) or Carbon or other Fiber depending on the Clinical Condition, which will then be rehabilitated in turn with a crown in the Ceramic League Aurea . |
| Fractures Under Bone Crest Therapy with Periodontal Bone Defects of Bi and Triforcations |
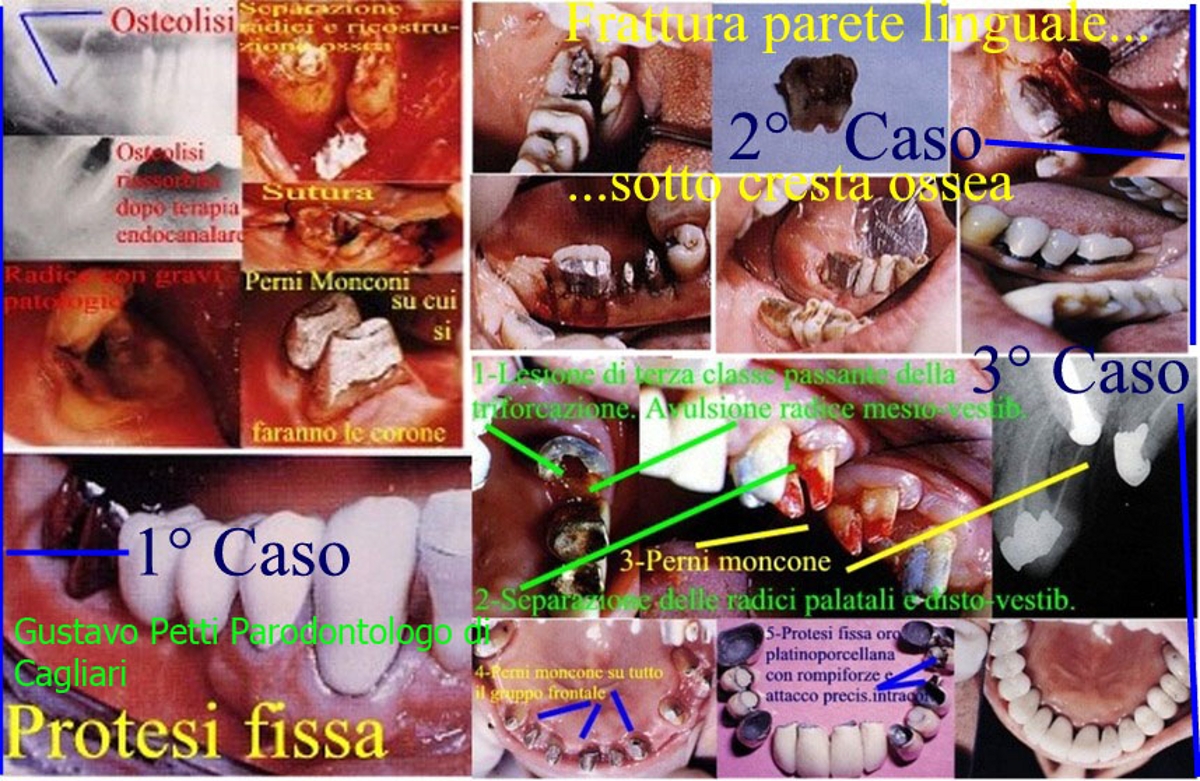
First Case: Fracture of the Lingual Wall of a lower Molar extending beneath the bony ridge in depth.
A Flap is Reposposed apically with PRP or PRF obtained from Centrifuged Blood of the Patient that acts as a "Glue" for the Lingual Lemo, with osteoplasty osteotomy to obtain the elongation of the Clinical Crown of the Tooth and "expose the whole Fracture zone" that will be so Treated endodontically and Rehabilitated with a Pin-Stump in turn rehabilitated with a Crown in Auric Alloy or in Zirconium Porcelain depending on the Clinical Situation!
Second Case: Fracture and Third Class Injury of Triforcation.
We proceed to the Surgical Avulsion of the Mesio-Vestibular Root with Severe Fracture of the Apical Third. The Palatal and Disto-Vestibular Roots are separated, the endodontically cured, and reconstructed with a single-abutment pin. We then proceed to the Deepening of the Barreling-in with a differentiated, very particular periodontal prosthetic preparation and rehabilitates it all with a fixed fixed prosthetic crown in the Aurea Preziosa (Gold-Platinum to have the right Elasticity and at the same time Hardness) taking care to insert a Rompi-Forces attack that connects them to the rest of the Prosthesis built entirely on Perni-Moncone di Radici which were all fractured under-Gingiva at the level of the Bone Cage.
Result is a COMPLETE ORAL REHABILITATION IN A COMPLEX CLINICAL CASE, in which Studio Petti is Specialized!

|
| Esthetic periodontal surgery |
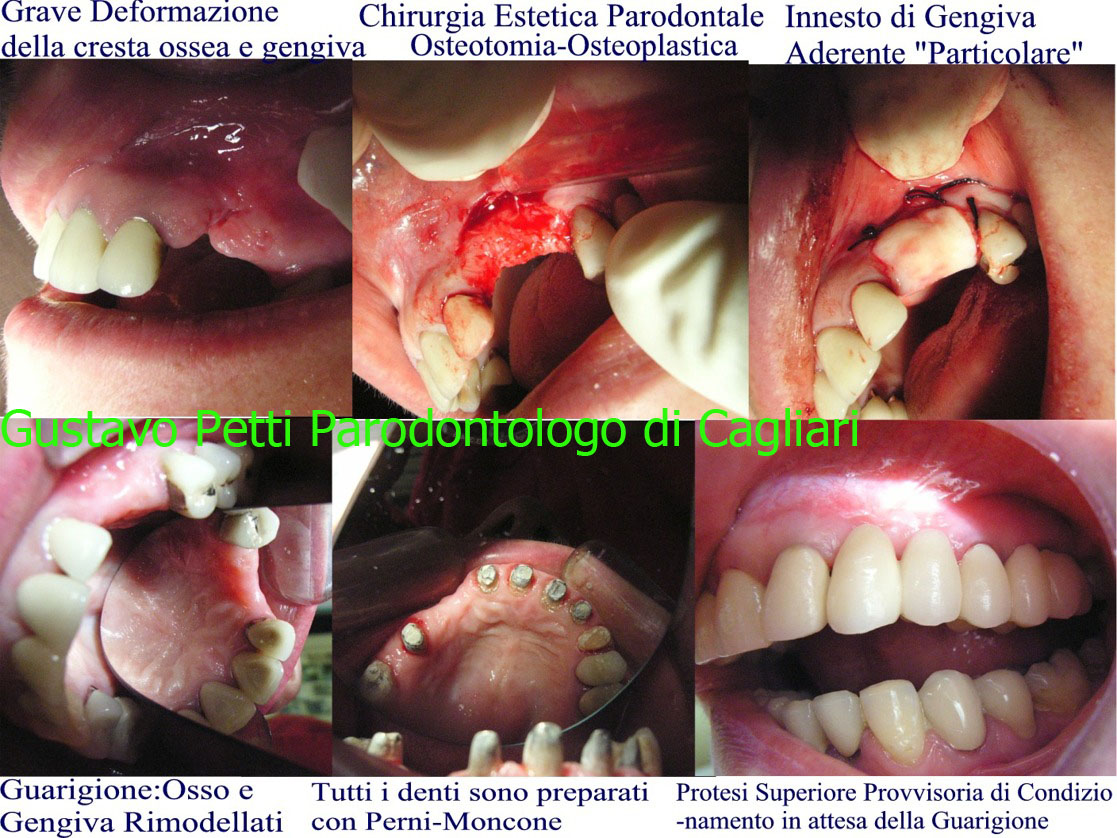
Severe Inestetism for Seria Deformation of the Ridge and Osseo and Gingiva Tablets:
One proceeds to Osteotomy-Osteoplasty for Remodeling the Bone and a Free Grafting of Keratinized Tissue to Reshape the Gingiva.
Other Teeth are saved with Perni-Moncone after Osteoplasty Diffuse Osteoplasty to expose all the fractured roots.
A Provisional Upper Provisional Prosthesis, Aesthetic Conditioning of Soft Tissues is built and Positions to have Harmony of Forms in the Relationships Crowns Prosthesis and Marginal Gingiva for an Ideal and Perfect Functional and Aesthetic Integration.
This is also a Case of Complete Oral Rehabilitation in a Complex Clinical Case in which Studo Petti is specialized! |