Published in March 1985
Externally chamfered gingivectomy in the treatment of hypertrophy caused by Dilantin sodium hyperplasia
GUSTAVO PETTI
Physician and Surgeon specializing in Dentistry. Periodontist.
Piazza Repubblica 4, 09129 Cagliari, Italy.
tel ++39 070 498159, fax ++39 070 400164
web site www.gustavopetti.it
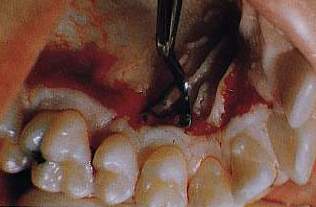
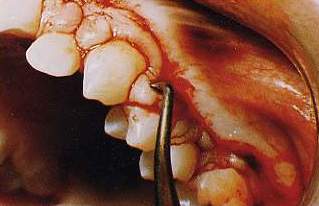
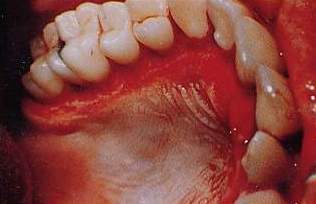
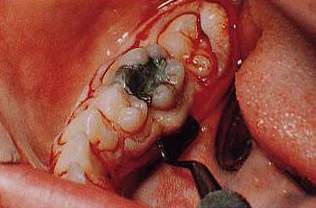
In cases in which the periodontal pocket does not go
beyond the mucogingival junction and sufficient adhering gum is available,
externally chamfered .

gingivectomy
is strongly indicated in the treatment of hypertrophy caused by Dilantin sodium hyperplasia
is strongly indicated in the treatment of hypertrophy caused by Dilantin sodium hyperplasia









References
A. Glickman, Clinical Periodontology, 1964
H.M. Goldman, D.W. Cohen, Terapia parodontale, 1962, 2, 885
B. Orban, Parodontologia - Concetti, teoria e pratica, 507-512,
1977
R.A. Yuodelis, D.H. Smith, La gengivectomia con bisello esterno,
La Clinica Odontoiatrica del Nord Am. vol. 9 n. 2, pag. 379, 380,
1979